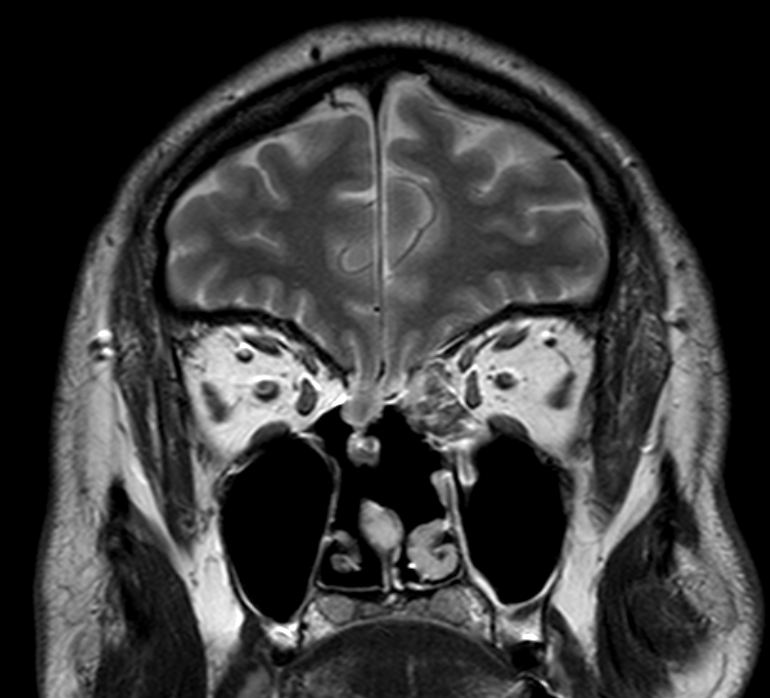
Nasal liquefaction is a condition in which there is a discharge of liquid (CSF) from the nasal cavity (perhaps also from the external ear canal, otoliquorrhea. In this case, transcranial surgery should be performed). The release of cerebrospinal fluid (nasal cerebrospinal fluid) becomes possible because there is a violation of the integrity of the bony structures of the base of the skull, as well as the integrity of the hard and soft meninges of the brain. Most often, as a result of a suffered craniocerebral injury, both in the early and in the remote periods. Nasal liquor accompanies meningocele (or meningoencephalocele), the latter represent a protrusion of the hard meningeal membrane of the brain with or without the brain substance towards the nasal cavity, paranasal sinuses. In the latter case, there is thinning of the membranes of the brain under the pressure of cerebrospinal fluid (with or without cerebrospinal fluid), which leads to the outflow of cerebrospinal fluid from this hernial sac – nasal cerebrospinal fluid. Nasal discharge can occur after surgery to remove tumors of the base of the skull, craniofacial tumors (both early and late). Quite often, nasal discharge occurs with an anomaly of the anatomical structure of the base of the skull (Sternberg’s canal). This leads to the emergence of complex types of nasal liquorrhoea or even meningocele in the lateral parts of the main sinus or the lateral pocket of the main sinus. Sometimes nasal discharge can occur spontaneously. Most often, this happens in people with excess weight, hypertension. Nasal liquors can differ in the intensity of secretions – from a couple of drops per day to constant secretions. They can differ in localization (nasal cavity, paranasal sinuses). Meningoencephalitis is a serious and serious complication of nasal discharge. Patients note several diseases of meningoencephalitis during one year. The diagnosis of nasal liquorrhoea is based on a laboratory study of liquid secretions from the nasal cavity. Subsequently, MSCT and MRI of the base of the skull are performed to verify the bone defect, meningocele, meningoencephalocele, and if necessary, CT cisternography with a contrast agent is performed, which shows the leakage of this contrast agent through the defect of the base of the skull into the nasal cavity. . Today, almost all nasal liquefies can be excluded (closed) by endoscopic endonasal (through the nasal cavity) access. The size of the bone defect, meningocele, meningoencephalocele, and their localization are of fundamental importance. In our department, we stopped the use of skull trepanation for the treatment of nasal liquorrhoea and only perform endoscopic endonasal surgical interventions. The treatment period is from 3-5 to 7-8 days.